
If you are reading this, there is a reasonable chance you are one of a relatively small group of people who has decided, often at some personal and professional cost, that the way medicine treats its own people is not good enough.
You have probably sat in a meeting where burnout was acknowledged in one breath and normalised in the next. You have watched colleagues quietly disintegrate under workloads that would be considered unacceptable in almost any other profession, while the institutional response amounted to a mindfulness leaflet and a reminder about the Employee Assistance Programme. You may have tried to raise the issue formally and found yourself navigating a culture that is, at best, politely resistant and, at worst, actively hostile to the conversation.
You are not imagining it… and you are not alone.
But I also want to say this clearly: what you are doing matters enormously, even when it doesn’t feel like it. In fact, especially when it doesn’t feel like it.
Because what you are doing, whether you use this language or not, is attempting to spread an idea through one of the most change-resistant professional cultures in existence. Understanding the science of how that process actually works may be one of the most practically useful things available to you right now.
The moment that changed the conversation
The COVID-19 pandemic placed doctors on the front line of a global crisis with inadequate protective equipment, shifting protocols, impossible decisions, and grief on a scale that most had never encountered in their professional lives. The moral injury was profound. The psychological toll was documented publicly, in real time. Doctors spoke openly about their mental health in ways the profession had historically discouraged. I wrote at the time about how the pandemic in many ways contributed to the dehumanisation of healthcare professionals, which had already been going on for a long time.
The public, for perhaps the first time, glimpsed what medicine had been quietly absorbing for decades, and they found it impossible to look away.
COVID did not create the doctor wellbeing crisis. It revealed it. The research had been building for years. Shanafelt and colleagues at Stanford had already established, through large-scale national surveys, that burnout among US physicians was not only prevalent but worsening, rising from 45.5% of physicians reporting at least one symptom in 2011 to significantly higher rates in subsequent years.¹ During the acute phase of the pandemic, that figure climbed to 62.8%, a level that made the pre-existing crisis impossible to attribute to individual frailty or insufficient resilience.² The data on physician suicide had been painting a sobering picture for longer still: a systematic review and meta-analysis of 25 studies found an overall standardised mortality ratio for physician suicide of 1.44 compared with the general population, with female physicians at nearly twice the risk of their male counterparts³. In Australia, the numbers were very similar, although there has not been any updated data since Beyond Blue conducted the last major study into the mental health of doctors and medical students in 2013.
These were not pandemic phenomena. They were pre-existing conditions that a global emergency finally made visible enough to demand a response.
That visibility matters, because it created something the science of change tells us is absolutely essential for an idea to move through a population- a critical mass of people who could no longer reasonably deny that there was a problem worth solving.
Why some ideas spread and others stall
In 1962, communication scholar Everett Rogers published Diffusion of Innovations, asking a question that turns out to be deeply relevant to anyone trying to shift medical culture: why do some ideas spread, and others stall?
Rogers found that when any new idea, behaviour, or practice enters a population, it doesn’t land evenly. It moves through five distinct groups, each with its own relationship to change, its own internal logic, and its own specific conditions that need to be met before adoption becomes possible. The speed at which something spreads depends not on the quality of the idea alone, but on how well it is understood, communicated, and supported at each stage of the journey.
Doctor wellbeing as a genuine clinical and institutional priority is, by any reasonable measure, still in the early stages of that journey within medicine. It has passionate advocates, a growing evidence base and the tailwind of a post-pandemic cultural shift that has made mental health discussion more acceptable across society. But it has not yet reached what Rogers would call critical mass within the profession itself, and understanding why requires an honest look at each of the five groups and what they actually need.
The five groups
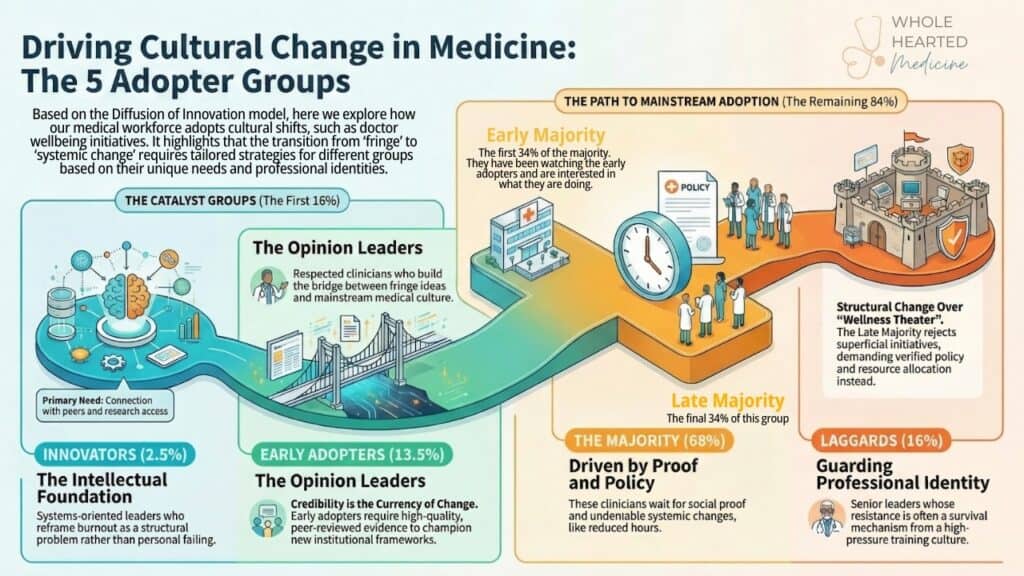
Innovators make up roughly 2.5% of the medical workforce. You probably know these people. You may, in fact, be one of them.
These are the clinicians, educators, and healthcare leaders who were talking about physician burnout, moral injury, and systemic cultural dysfunction in medicine long before it was a safe or particularly popular thing to do. They were writing about it in journals, raising it in meetings, building programmes with limited resources and even more limited institutional support, and absorbing the professional scepticism that often greets those who name uncomfortable truths in hierarchical organisations.
One of the most important early contributions from this group came from Shanafelt and Noseworthy, whose landmark 2017 paper in Mayo Clinic Proceedings argued that physician burnout is fundamentally a system issue, not an individual one, and that approximately 80% of the challenge is driven by characteristics of the work environment and organisational culture rather than by deficits in individual resilience.⁴ That reframe, from personal failing to structural problem, is the intellectual foundation on which the entire doctor wellbeing movement now rests. It took innovators to put it into the literature.
Innovators are intellectually driven, systems-oriented, and comfortable operating on the fringe of accepted discourse. They don’t need consensus before they act. They need evidence, a problem worth solving, and enough conviction to keep moving when the culture pushes back.
If this is you, your role in this movement is irreplaceable. You are the reason the conversation exists at all. But it is worth naming something that innovators in any field sometimes struggle with: the skills that make you exceptional at identifying and championing a new idea are not always the same skills required to bring a sceptical majority along with you. That is not a failing. It is simply a different part of the work, and it may require different tools and different allies. Connection with other innovators, access to robust research, and strategic support in translating visionary advocacy into institutional change are not luxuries for this group- they are necessities.
Early adopters make up around 13.5% of the medical workforce, and they are arguably the most important group for anyone trying to shift medical culture.
These are the clinicians, and perhaps the department heads, medical educators, or healthcare executives, who are not yet publicly championing doctor wellbeing but are privately persuaded that something needs to change. They have watched colleagues burn out. They have their own quiet history with the cost of the culture. They are paying close attention to what the innovators are doing.
What distinguishes early adopters from innovators is deliberation. They need to see credible evidence before they act, and they need to feel that acting will not significantly damage their professional standing. In a culture as reputation-conscious as medicine, that second condition is not trivial. Once early adopters are genuinely convinced though, they carry enormous weight. These are the opinion leaders, the people medical institutions actually listen to.
When a respected clinician speaks openly about their own experience of burnout, it does more for cultural change than a hundred advocacy documents. When a clinical director integrates protected wellbeing time into a department’s structure, colleagues in other departments notice. When a medical school dean makes faculty and student wellbeing a visible institutional priority, it signals to the entire organisation that this is now a legitimate concern.
COVID accelerated the movement of many in this group into more active positions. The pandemic gave early adopters the social permission and the undeniable evidence they needed to step forward.
At Whole Hearted Medicine, we see this group clearly and consistently. Over six years and nearly 30 retreats, the majority of the more than 400 doctors who have come to us from across Australia and New Zealand have been early adopters. These are clinicians who arrived already persuaded that something needed to change, both within themselves and within their profession. What they were looking for was not more information- it was connection, community, and a structured space to translate their conviction into something they could carry back into their working lives.
Many of them have done exactly that. They have taken their energy, their insight, and their renewed sense of purpose back into hospitals, practices, and medical schools, and created what I can only describe as ripples. That is the early adopter doing what Rogers always said they do best, building the bridge between the fringe and the majority.
What early adopters need most is high-quality, peer-reviewed evidence they can cite with confidence, institutional frameworks they can adopt without reinventing from scratch, and the visible support of credible professional bodies. They need to know that moving on this will not cost them more than it gains.
The early majority represent around 34% of the medical workforce, and this is the group that will determine whether doctor wellbeing becomes genuinely embedded in medical culture or remains a peripheral conversation among committed advocates.
These are the clinicians and healthcare professionals who are aware of the wellbeing agenda, probably sympathetic to it in principle, but not yet doing anything meaningfully different as a result. They are watching, and they are weighing up the information and options available to them. They are looking for social proof that change is both possible and professionally safe.
This group responds to lived experience above abstract argument. A colleague who has completed a structured wellbeing program and returned visibly different. A ward culture that has genuinely shifted and whose clinical and human outcomes have improved as a result. A cohort of medical students who have been through a curriculum redesigned with wellbeing at its core, and who are entering the profession in better shape than their predecessors.
The early majority are not waiting for someone to convince them intellectually. They are waiting for enough people around them to make the change so that it starts to feel normal rather than exceptional.
Something I find genuinely encouraging is that at our retreats, we are now seeing a growing number of doctors who sit squarely in this early majority. These are clinicians who, a few years ago, might not have considered attending. What has brought them is exactly what Rogers’ model would predict: they have watched someone they respect, a colleague, a registrar, a friend from training, come back from one of our retreats changed in some visible and credible way. The social proof is beginning to accumulate. The tipping point, while not yet reached, feels closer than it did.
The late majority are also around 34% of the medical workforce, and many of them have earned their scepticism.
These are the clinicians and leaders who have watched wellness initiatives come and go. They have seen the yoga class added to the staff intranet, the resilience workshop offered in response to a 70-hour working week, the wellbeing survey administered during the most pressured period of the year. They have experienced wellness as performance, as box-ticking, as a way of managing the optics of a broken system without addressing its structural failures.
Their resistance is not irrational. It is, in many cases, the appropriate response to years of being offered the wrong solution to the right problem. The research is clear that individual-level interventions alone are insufficient to address what is, at its core, a systemic issue. As Shanafelt and Noseworthy articulated so precisely, burnout cannot be solved by asking individuals to be more resilient within structures that remain unchanged.⁴
What will reach this group is not more advocacy. It is structural, visible, undeniable change.
- Reduced working hours.
- Protected time for clinical supervision and peer support.
- Genuine psychological safety in reporting errors and expressing distress.
- A hiring and promotion culture that values whole doctors rather than simply productive ones.
When the late majority see that the institution itself has changed, not just its language, they will begin to move. That is a high bar. It is, however, the correct bar.
Laggards make up around 16% of the medical workforce, and I think it would be a mistake to not spend enough time here considering what this important group need.
These are not simply obstructive people. Many are doctors who have survived a demanding career by building a particular internal architecture around endurance, self-sufficiency, and the suppression of emotional and physical need. That architecture did not emerge from weakness. It emerged from a training culture that rewarded it, and in some cases required it for survival.
When you ask someone who has built their professional identity on not needing support to embrace a culture of psychological openness, you are not asking them to adopt a new habit. You are asking them to revise a core part of how they understand themselves as a doctor. That is not a small thing.
Laggards in this space also often hold seniority. Their visible resistance, whether through active opposition or simply the modelling of the old culture, carries significant weight in departments and institutions where hierarchy matters. The approach that works here is not confrontation. It is patient, respectful engagement that does not require explicit conversion. Often, the goal is simply to reduce active opposition and create space for the culture around them to shift. Sometimes, with time and the right relationships, more than that becomes possible. What this group needs, above all else, is to have their professional experience honoured rather than dismissed, and to be engaged in ways that do not threaten their identity or their legacy.
What this asks of you
If you are a changemaker in medicine, this framework asks something beyond passion and conviction. It asks you to be strategic about where you invest your energy, who you are speaking to at any given moment, and what that person actually needs from you to move.
It asks you to recognise that
- Innovators need community and protection from the isolation that comes with being ahead of the curve.
- Early adopters need credible evidence and institutional permission.
- Early majority need to see change working in real people’s lives before they will risk joining it.
- Late majority need structural proof, not persuasion; and
- Laggards need patient respect, not conversion.
Over the past six years, I have watched something quite specific happen. Doctors arrive on our retreats carrying the weight of a culture that has taken a great deal from them. Yet, here they are ready to invest in connection, in learning, in growth, despite that. In reverence of this, what we have always aimed to cultivate through Whole Hearted Medicine, is hope. Hope that is grounded in community rather than in isolation.
That hope travels back into workplaces. It shows up in conversations that wouldn’t otherwise have happened, in small structural changes that someone finally felt equipped to advocate for, in a registrar who watched their supervisor model vulnerability and filed it away as permission to do the same. That hope and connection is the all-important fuel for the changemakers of medicine to keep doing what they are doing. To “be the change (they) wish to see in the world”.
More recently, through our Whole Hearted Leadership retreats delivered in collaboration with Capstan Partners, we have extended this work specifically to medical leaders, equipping them with coaching skills and leadership frameworks that allow them to amplify their commitment to doctor wellbeing within their sphere of institutional influence. In Rogers’ terms, this is a direct investment in the early adopter and early majority interface. It is how we accelerate the spread. Not by pushing harder, but by equipping the right people with the right tools to lead from where they already stand.
It is also, I’ll be honest, one of the most professionally fulfilling things I have been part of in my life.
Because the theory tells us that every group eventually moves. The innovators and early adopters are already in motion. The early majority are watching closely and, increasingly, stepping forward. The late majority will follow when the culture shifts enough to carry them. Even laggards, when given enough time and the right conditions, adapt.
You are not pushing against something immovable. You are pushing against something that moves slowly, and that is a very different thing.
Keep going.
Dr Emily Amos is a General Practitioner experienced in mindfulness, meditation, lifestyle medicine and stress management, and the Director of Whole Hearted Medicine. She works with clinicians, healthcare organisations, and medical educators across Australia and New Zealand to build evidence-informed, sustainable approaches to practitioner wellbeing.
👉 Learn about Whole Hearted Medicine
References
- Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172(18):1377-1385. doi:10.1001/archinternmed.2012.3199
- Shanafelt TD, West CP, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clin Proc. 2022;97(12):2248-2258. doi:10.1016/j.mayocp.2022.09.002
- Dutheil F, Aubert C, Pereira B, et al. Suicide among physicians and health-care workers: a systematic review and meta-analysis. PLoS ONE. 2019;14(12):e0226361. doi:10.1371/journal.pone.0226361
- Shanafelt TD, Noseworthy JH. Executive leadership and physician well-being: nine organisational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2017;92(1):129-146. doi:10.1016/j.mayocp.2016.10.004